GLP-1 receptor agonists (like semaglutide — Ozempic/Wegovy — and related medications) have changed the conversation around obesity and metabolic health. Many people now see significant weight loss in a relatively short time.
But there’s an important detail that doesn’t show up on the scale:
Rapid weight loss can include meaningful lean mass loss (fat-free mass), and a portion of that can be skeletal muscle.
For adults 40+, and especially older adults, this matters deeply because muscle is not just “fitness” — it’s foundational to mobility, metabolism, insulin sensitivity, and long-term independence.
At MobiGym, our focus is not “weight loss at all costs.”
Our goal is healthy weight loss: reduce fat while preserving (and ideally improving) strength, muscle, function, and metabolic resilience — especially when GLP-1 therapy is part of the picture.
What is GLP-1?
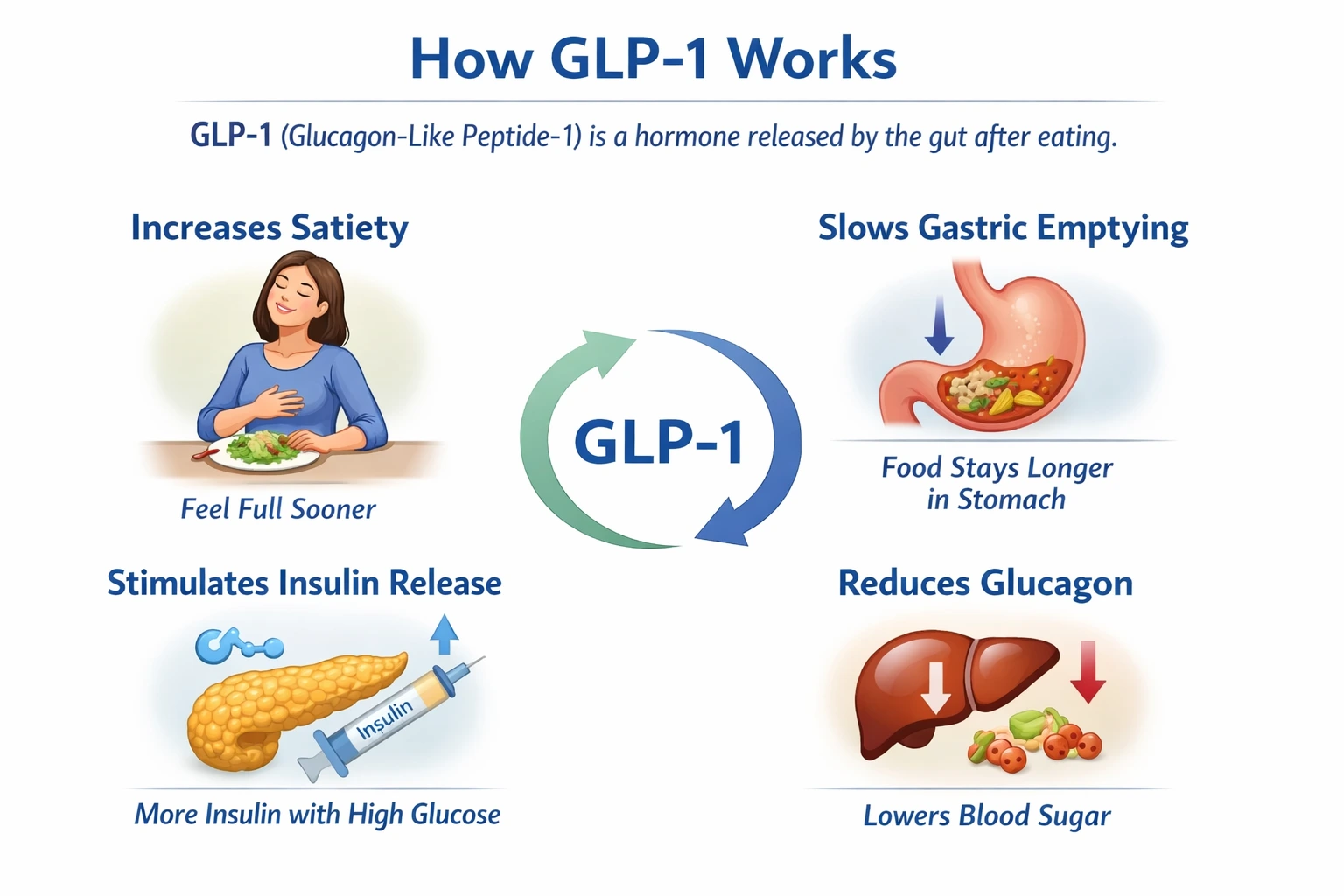
GLP-1 (Glucagon-Like Peptide-1) is a natural hormone released by the gut after you eat. It helps regulate appetite and blood sugar by:
Increasing satiety (you feel full sooner)
Slowing gastric emptying (food stays longer in the stomach)
Stimulating insulin release when glucose is elevated
Reducing glucagon (a hormone that raises blood sugar)
GLP-1 receptor agonist medications mimic this natural hormone — but with a much longer half-life, meaning they stay active in the body far longer than your natural GLP-1 surge after a meal.
That’s why people often report:
Less hunger / “food noise”
Smaller portions
Easier adherence to a calorie deficit
Why do GLP-1 drugs often lead to lean mass loss?
A key principle of fat loss physiology:
Most weight loss methods reduce both fat mass and fat-free mass. The faster the loss and the bigger the deficit, the more this becomes an issue.
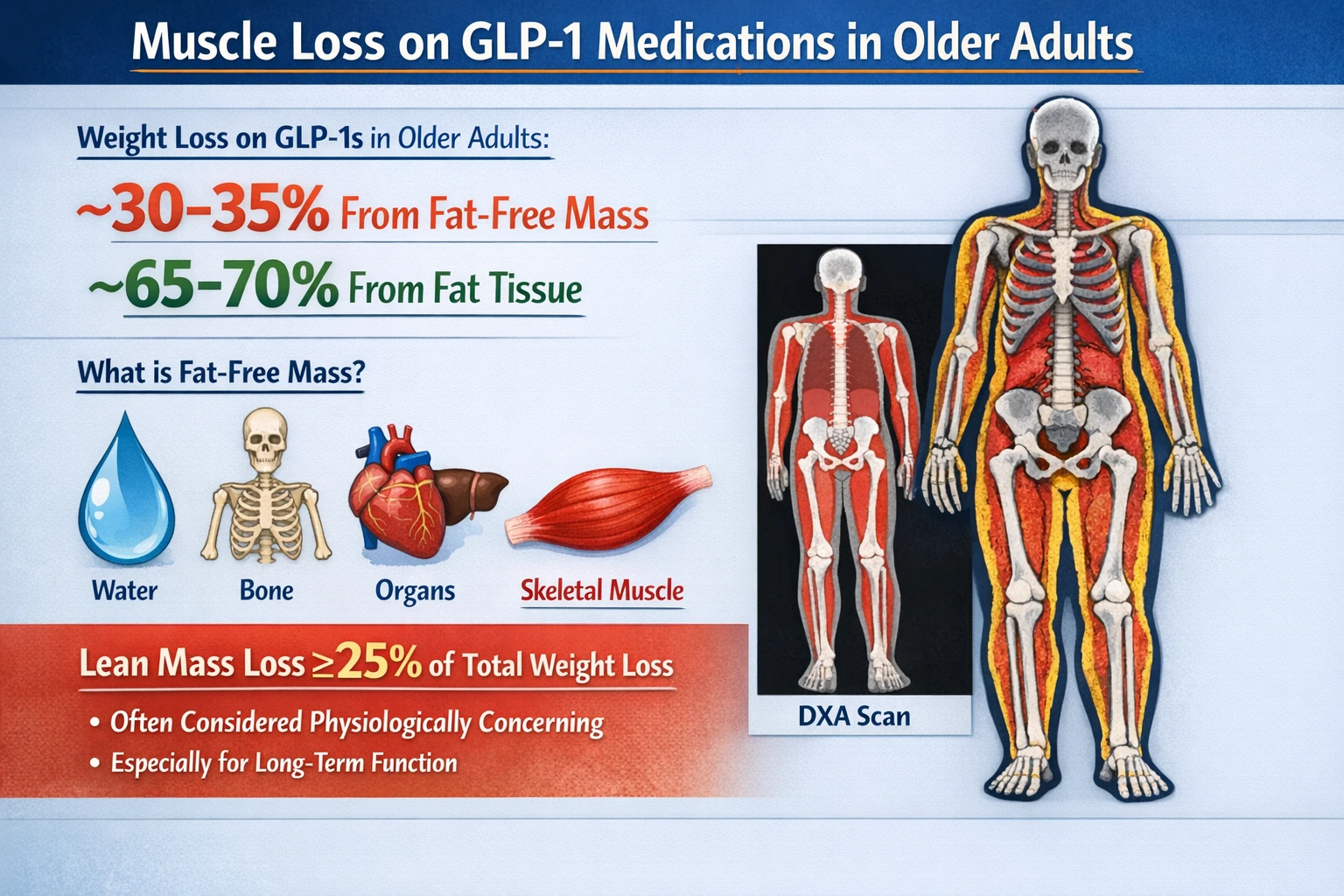
From the emerging data highlighted in recent clinical discussions:
In older adults using GLP-1s, weight loss may include roughly 30–35% from fat-free mass, with the remainder primarily fat.
“Fat-free mass” on DXA includes water, bone, organs, and skeletal muscle — and skeletal muscle makes up a large portion of that compartment.
Lean mass loss ≥25% of total weight loss is often considered physiologically concerning, especially for long-term function.
This matters even more because after 40, many adults already trend toward age-related muscle loss over time — and GLP-1-associated weight loss can accelerate that trajectory if not counterbalanced properly.
Why muscle loss is the hidden “cost” of weight loss
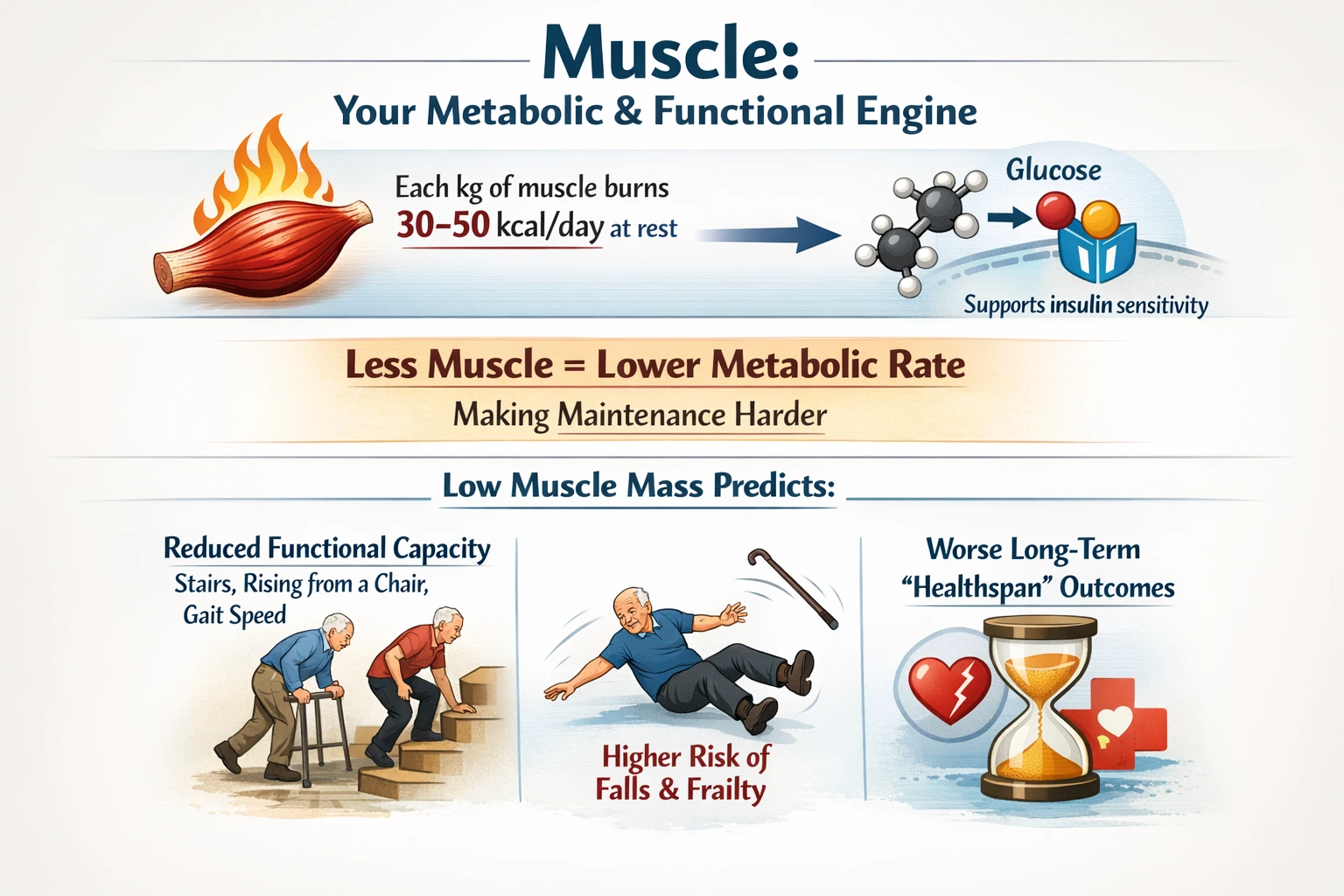
Muscle is your metabolic and functional engine:
Each kilogram of muscle burns roughly 30–50 kcal/day at rest
Muscle increases glucose uptake → supports insulin sensitivity
Less muscle can mean lower metabolic rate, making maintenance harder
Low muscle mass predicts:
reduced functional capacity (stairs, rising from a chair, gait speed)
higher risk of falls and frailty
worse long-term “healthspan” outcomes
In other words:
If the scale goes down but strength and function go down with it, that’s not a win.
The MobiGym perspective: “Weight loss” vs “Body Recomposition”
GLP-1 medications can be a tool.
But the body outcome depends heavily on the strategy you run alongside it.
At MobiGym, we specialize in body recomposition, meaning:
✅ Fat loss as the priority
✅ Lean mass preservation as the safeguard
✅ Strength, performance, energy, and function as the real KPIs
✅ Lifestyle integration (sleep, stress, recovery, protein, training quality)
✅ Continuous measurement and adjustment
If medication is part of your plan, we build a training + nutrition strategy that respects:
lower appetite
lower total food volume tolerance
fatigue variability
GI side effects
recovery capacity
Most important contraindications and cautions (talk to your clinician)
This section is educational and not medical advice — always confirm with your prescribing clinician.
GLP-1 receptor agonists are commonly contraindicated or used with special caution in people with:
Personal or family history of medullary thyroid carcinoma (MTC)
Multiple Endocrine Neoplasia syndrome type 2 (MEN2)
Pregnancy / breastfeeding (typically avoided)
History of pancreatitis (often caution / case-by-case)
Gallbladder disease risk (rapid weight loss can increase gallstone risk)
Severe GI conditions (because these drugs can worsen nausea, vomiting, delayed gastric emptying)
Certain medication combinations or medical conditions that require careful monitoring
Common side effects can include:
nausea, constipation/diarrhea, reflux
reduced energy intake (which is exactly why protein and strength training become crucial)
How to protect muscle on GLP-1 therapy: the 3 pillars

1) Resistance training (2–3×/week)
Progressive resistance training is the #1 lever to protect muscle during weight loss.
At MobiGym, we build plans around:
safe but progressive loading
compound movement patterns (push, pull, hinge, squat, carry)
joint-friendly regressions and intelligent progression
measurable strength targets over time
Even older adults can improve strength and muscle with the right program design and progression.
2) Protein (typically 1.2–1.6 g/kg/day)
This range is widely used in the evidence base for supporting muscle retention during fat loss.
Practical structure (often easier on GLP-1):
Protein-first meals
2–3 protein feedings/day, sized to tolerance
consistent protein after training (recommended, not mandatory)
If appetite is very low, we prioritize protein as the “non-negotiable.”
3) Monitoring and adjustment (don’t guess)
The scale is not enough.
We typically track:
body composition (fat mass vs lean mass trend)
strength performance and training quality
waist/hip measures (and waist-to-height trend)
fatigue, recovery, sleep, digestion
If strength drops for 2+ weeks or fatigue is persistent, we adjust:
training load and recovery
protein intake strategy
total energy intake timing
lifestyle constraints (stress, sleep, work travel)
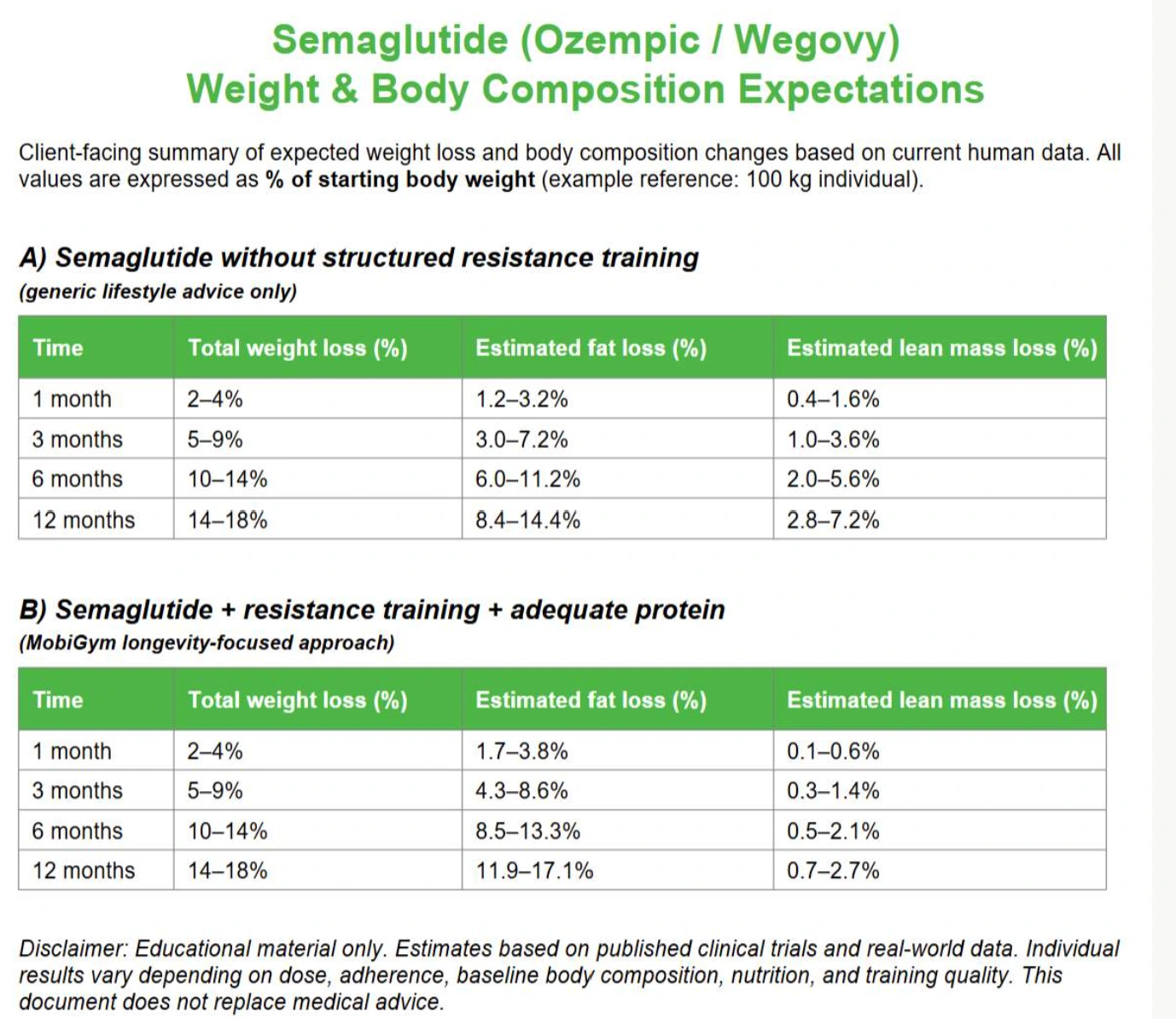
What results can you expect with the MobiGym approach?
When GLP-1 use is paired with:
structured resistance training
adequate protein
smart recovery and monitoring
…the goal is to shift weight loss toward:
more fat loss
less lean mass loss
better strength retention
better long-term maintenance
This is exactly why we built our MobiGym comparison framework:
Same medication. Different outcomes — depending on training and nutrition strategy.
A simple starting plan (that we personalize at MobiGym)
If you want a simple baseline (to discuss with your coach and clinician):
Strength training: 2 sessions/week, non-consecutive
Protein: aim for 1.2–1.6 g/kg/day (as tolerated)
Daily movement: walking or low-impact cardio most days (10–30+ minutes)
Hydration + fiber: support digestion and constipation risk
Optional: creatine 3–5 g/day with clinician approval, especially helpful when paired with strength training
Bottom line
GLP-1 medications can be life-changing for weight loss.
But muscle is not optional — it is foundational.
If you’re on Ozempic/Wegovy (or considering it), the smartest move is to treat medication as one part of a complete body recomposition strategy.
At MobiGym, we specialize in integrating training, nutrition, lifestyle, and (when present) medication context — to protect what matters most: strength, function, and healthspan.
Call to action
Want a personalized plan that aligns GLP-1 therapy with body recomposition?
DM MobiGym or book a discovery session to review:
your starting body composition
your lifestyle constraints
your training history and risks
your protein strategy
your short- and long-term goals
Disclaimer
This article is educational information only and does not replace medical advice. Always consult your physician or prescribing clinician before starting, stopping, or changing any medication, supplement, or exercise program. Training and nutrition should be individualized. Results may vary based on dose, adherence, baseline body composition, nutrition, sleep, stress, medical history, and training quality.